

Fertility Rate in Central Visayas is 2.0
In the Philippines, fertility has decreased substantially since 1993 with a total fertility rate at 4.1 to 2.7 in 2017 but it then decreases to 1.9 children per woman in 2022. Central Visayas fertility rates among women also decreased substantially from 4.4 in 1993 and 2.0 in 2022. Furthermore, in 2022, women in Central Visayas have an average of 2.0 children per woman. (Figure 1)

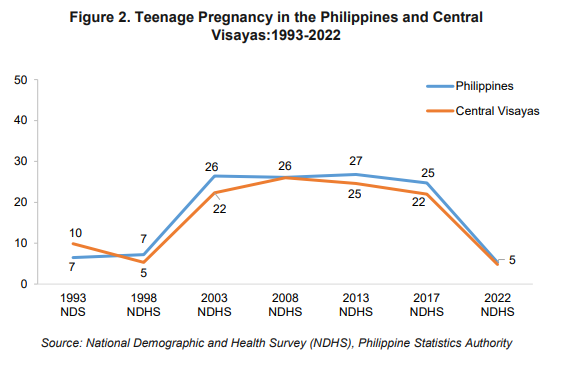
Teenage Pregnancy in Central Visayas is 5 percent
In Central Visayas, the percentage of women age 15-19 years who have ever been pregnant is 5 percent in 2022. This is lower by 78 percent compared to the 2017 results which is 22 percent. In 2022, percentage of women age 15-19 years in the Philippines who have ever been pregnant is also 5 percent. (Figure 2)
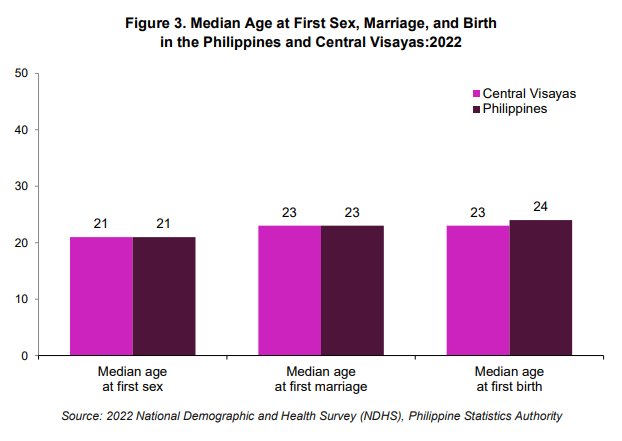
Median Age at First Sex, Marriage, and Birth
In 2022, women age 25-49 in Central Visayas initiate their first sexual intercourse at a median age of 21 years. The median age at first marriage for Filipino women is 23 years, this is two years older than the median age at first sexual intercourse. The same trend was also observed in the Central Visayas. Childbearing in the Philippines comes within one (1) year of marriage where the median age at first birth is 24 years while in Central Visayas, the median age at first birth is 23 years. (Figure 3)
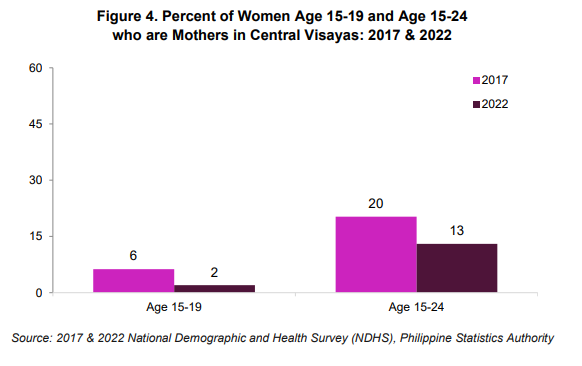
Early Pregnancy and Motherhood in Central Visayas is 2 percent
In Central Visayas, the percentage of young women age 15-19 who are mothers decreases from 6 percent in 2017 to 2 percent in 2022. Also, the trend for women age 15-24 who are mothers decreased from the result in 2017 at 20 percent to 13 percent in 2022. (Figure 4)
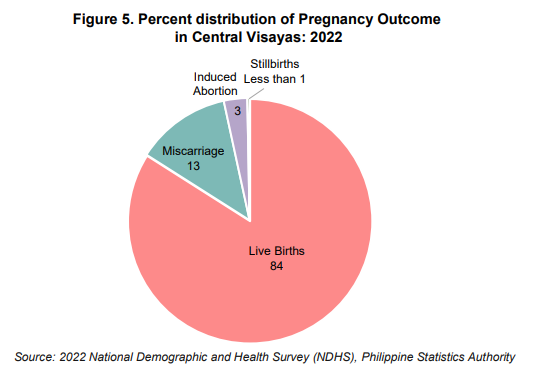
Pregnancy Outcomes in Central Visayas
In Central Visayas, 84 percent of pregnancies in the three years before the survey resulted in live births, while 13 percent were miscarriages, less than 1 percent (0.3%) were stillbirths, and 3 percent were induced abortions. (Figure 5)
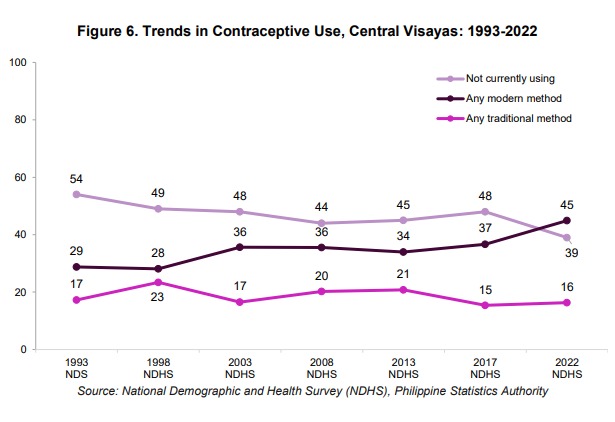
Trends in Contraceptive Use in Central Visayas
The use of modern methods of family planning among married women in Central Visayas has steadily increased over the last two decades, from 36 percent of married women in 2003 to 45 percent in 2022. However, married women’s use of traditional methods of family planning has remained relatively stable with 16 percent of married women using traditional methods of family planning in 2022. (Figure 6)
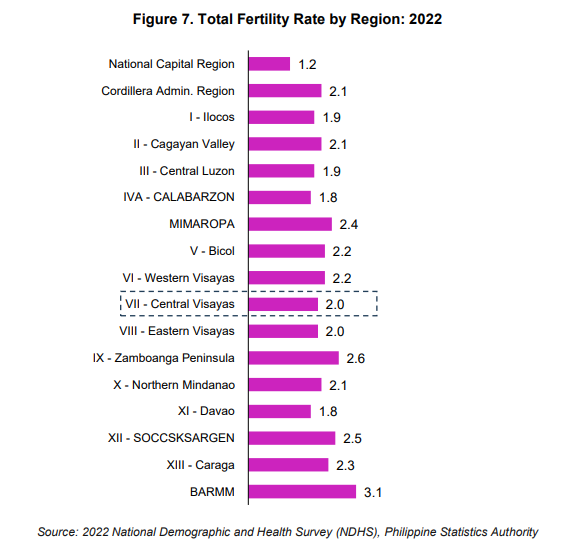
Central Visayas ranks 4th with lowest Total Fertility Rate across Regions
Comparing the Total Fertility Rate with Modern Contraceptive Prevalence Rate across regions, BARMM reported the highest TFR at 3.1 children per woman in 2022. Central Visayas ranked 4th with the lowest TFR. (Figure 7)
Demand for Family Planning among Married Women
In Central Visayas, 61 percent of married women have a met need for family planning which means they are using any method of family planning. Meanwhile, 13 percent of married women have an unmet need for family planning which means they are not currently using family planning, but do not wish to become pregnant for at least 2 years, if at all. The remaining 26 percent of married women do not have a need for family planning, which means that they do not wish to delay or limit pregnancy.
(Figure 8)

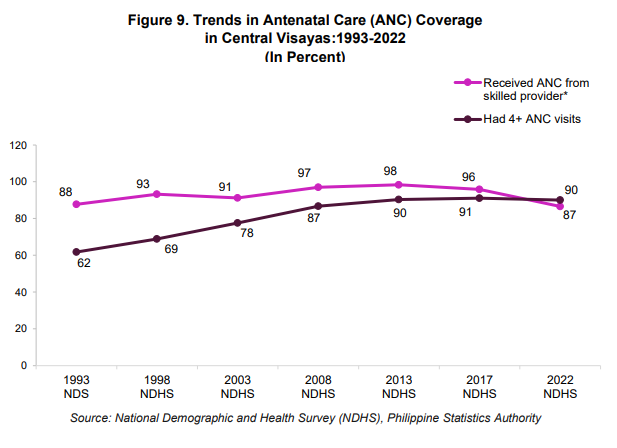
Antenatal Care (ANC) Coverage in Central Visayas
Antenatal care or pregnancy care is a preventive healthcare provided by health care professionals to pregnant women to prevent complications during pregnancy and even maternal and child deaths.
In Central Visayas, the percentage of women with a live birth in the 2 years preceding the survey who received antenatal care from a skilled provider increased from 88 percent in 1993 to 98 percent in 2013 before decreasing to 87 percent in 2022. On the other hand, the percentage of women with a live birth who had more than 4 ANC visits during their pregnancy increased from 62 percent in 1993 to 90 percent in 2022. (Figure 9)
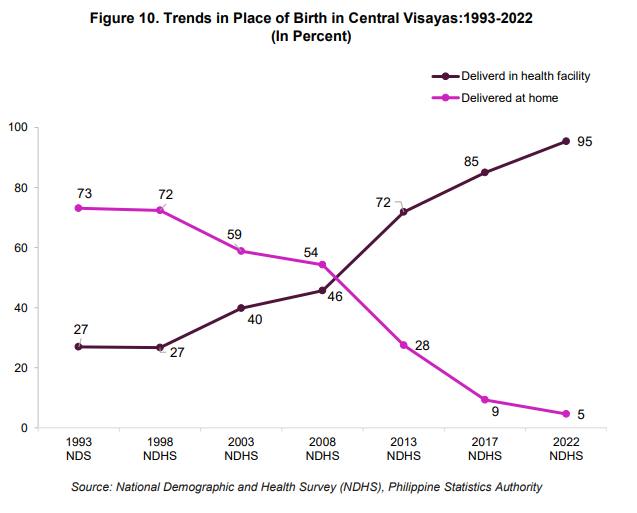
Trends in Place of Birth in Central Visayas
Giving birth at a hospital with skilled assistance reduces the risk of compromising women’s health as well as that of their newborns. Health facility-based deliveries in Central Visayas have more than tripled over the past 3 decades, from 27 percent of live births in 1993 to 95 percent in 2022. Over the same period, the proportion of live births delivered at home has dramatically decreased from 73 percent to 5 percent. (Figure 10)
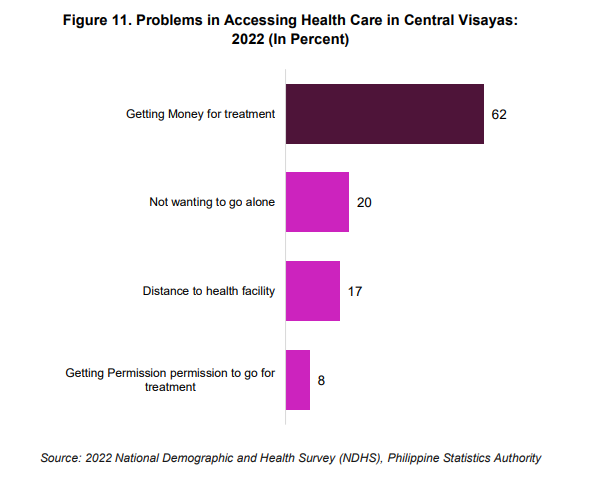
Problems in Accessing Health Care in Central Visayas
Women were asked whether each of the following factors is a big problem in seeking medical advice or treatment for themselves when they are sick such as getting money for treatment, not wanting to go alone, distance to health facility and getting permission to go for treatment.
In Central Visayas, getting money for treatment is the most common problem in accessing healthcare with 62 percent followed by not wanting to go alone with 20 percent and distance to health facility with 17 percent. (Figure 11)
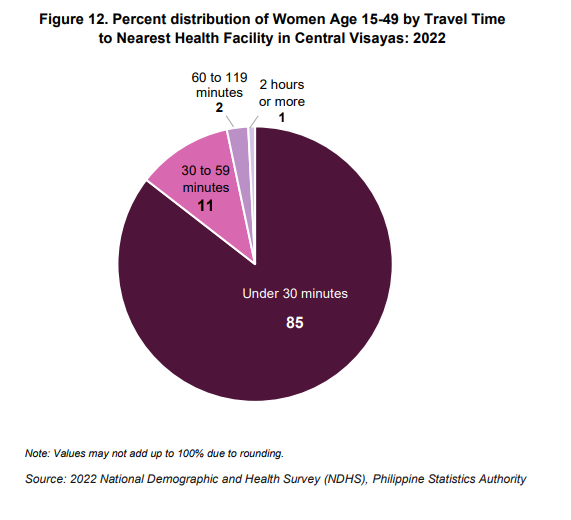
Distance from Healthcare Facility in Central Visayas
About 85 percent of women in Central Visayas reported that the travel time from their home to the nearest health facility is less than 30 minutes. Only 1 percent indicated that their travel time is 2 hours or more. (Figure 12)
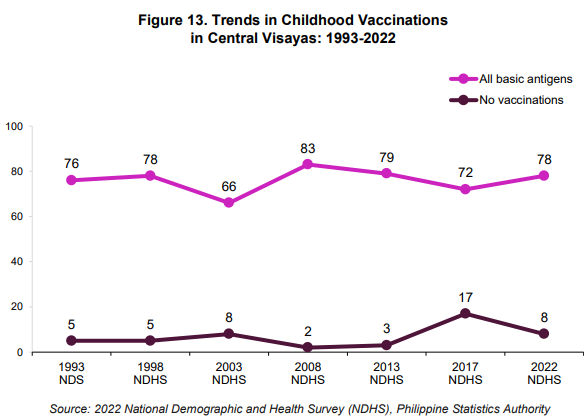
Trends in Childhood Vaccinations in Central Visayas
In Central Visayas, 78 percent of children age 12-23 months received all basic antigens. Basic antigen coverage increased from 76 percent in 1993 to 83 percent in 2008, before decreasing to 79 percent in 2013 and has yet to regain the peak in vaccination coverage observed in 2008. (Figure 13)
Children age 12-23 months who did not receive any vaccination decreased from 5 percent in 1993 to 3 percent in 2013 and erratically increased in 2017 at 17 percent. However, it was decreased in 2022 with 8 percent.
Basic antigens include one dose of BCG, three doses of polio vaccine, three doses of DPT-containing vaccine, and one dose of MMR or measles mump rubella. (Figure 13)
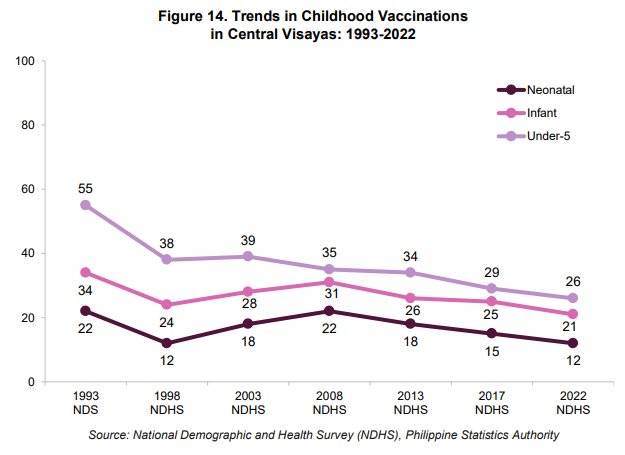
Trends in Childhood Mortality in Central Visayas
Childhood mortality in Central Visayas declined from 1993 to 1998, but the progress stalled in 2017, as all three childhood mortality rates are essentially unchanged from 2017 to 2022.
For the 10-year period before the survey in 2022, there were 12 children died in the first month of life per 1,000 live births. This is neonatal mortality. Infant mortality in Central Visayas is 21 children dying in the first year of life per 1,000 live births. The under-5 mortality rate is 26 deaths before age 5 per 1,000 live births. (Figure 14)
Knowledge of HIV/AIDS in Central Visayas
In 2022, 93 percent of Filipino women age 15-49 have heard of HIV or AIDS. In Central Visayas, the percentage of women age 15-49 years who have heard of HIV or AIDS is higher than the national figure at 95 percent. (Figure 15)
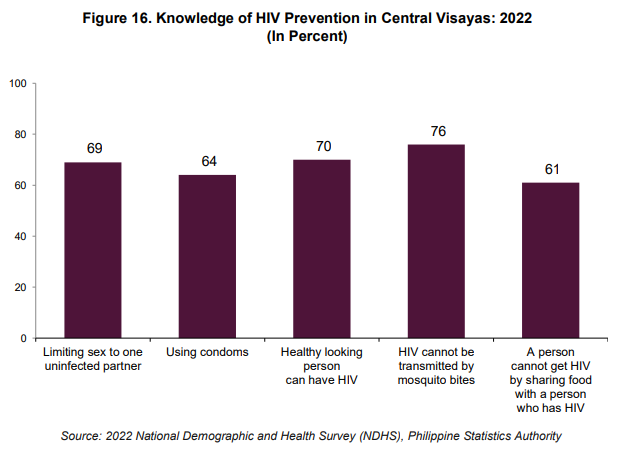
Knowledge of HIV Prevention in Central Visayas
Knowledge of how HIV is transmitted is crucial in enabling people to avoid HIV infection, and this is especially true for young people, who are often at greater risk because they may have shorter relationships with more partners or engage in other risky behaviors.
In Central Visayas, 76 percent of women age 15-49 years know that HIV cannot be transmitted by mosquito bites, 70 percent know that a healthy-looking person can have HIV, and 69 percent know that limiting sex to one uninfected partner can prevent HIV. (Figure 16)
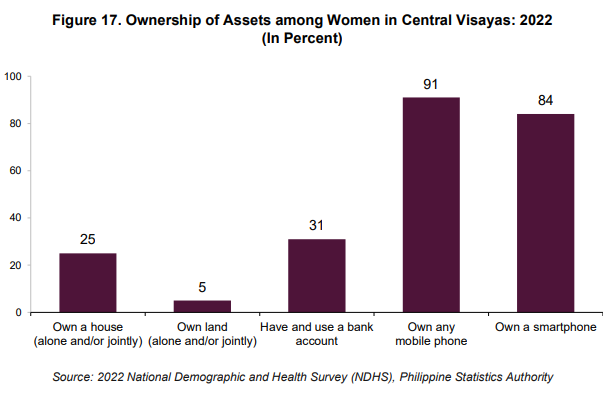
Ownership of Assets among Women in Central Visayas
One-fourth of women in Central Visayas own a house alone or jointly with a partner/husband. Similarly, 31% of women in Central Visayas have and use a bank account. And, 4 in 5 women have a mobile phone or smartphone. (Figure 17)
Women’s Participation in Decision Making in Central Visayas
Women are considered to participate in household decisions if they make decisions alone or jointly with their husband in all three of the following areas:
(1) their own health care,
(2) major household purchases, and
(3) visits to their family or relatives.
In Central Visayas, nine in ten of married women participate in decisions about their own health care and visits to their family or relatives. (Figure 18)
Eighty-nine percent of women participate in decisions about making major household purchases, 86 percent of women participate in all three decisions and only one percent participate in none of the three decisions. (Figure 18)

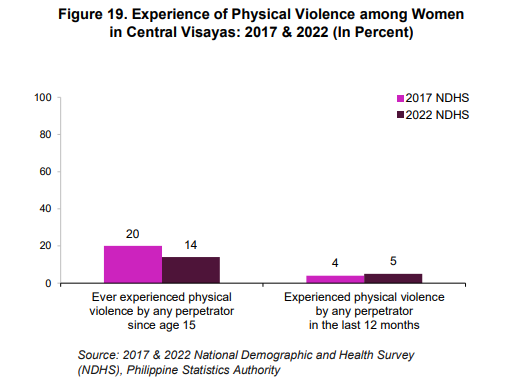
Experience of Physical Violence in Central Visayas
Women in Central Visayas who have ever experienced physical violence since the age of 15 decreased from 20 percent in 2017 to 14 percent in 2022. While women who have experienced physical violence in the last 12 months preceding the survey increased by one percent in 2022. (Figure 19)
Approved by:
(SGD.) ARIEL E. FLORENDO
Regional Director
TECHNICAL NOTES
2022 National Demographic and Health Survey
I. Introduction
a. Background
The 2022 Philippine National Demographic and Health Survey (NDHS) is the seventh Demographic and Health Survey (DHS) conducted in the Philippines in collaboration with the worldwide Demographic and Health Surveys Program, and the 12th in a series of national DHS conducted every five years since 1968.
The 2022 NDHS was implemented by the Philippine Statistics Authority (PSA). ICF provided technical assistance through The Demographic and Health Survey Program (DHS), which is funded by the United States Agency for International Development (USAID) and offers financial support and technical assistance for population and health surveys in countries worldwide.
b. Objectives
The primary objective of the 2022 NDHS is to provide up-to-date estimates of basic demographic and health indicators. Specifically, it gathers information to provide indicators on fertility, fertility preferences, family planning practice, childhood mortality, maternal and child health, nutrition, knowledge and attitudes regarding HIV/AIDS, violence against women, child discipline, early childhood development, and other health issues. These indicators are crucial in policymaking, program planning, and monitoring and evaluation of population and health programs, including those related to the Sustainable Development Goals (SDGs).
c. Scope and coverage
The 2022 NDHS has a national sample of approximately 35,000 sample households and 28,000 women aged 15-49 deemed sufficient to provide reliable estimates at the national and regional levels. All the eligible women 15-49 years old in the sample households were interviewed including those visitors who stayed the night before the interview. One eligible woman per household selected for the Woman’s Safety Module, one child aged 1-14 per household selected for Child Discipline Module, and one child aged 2-4 per eligible woman selected for Early Childhood Development Index Module.
These sample housing units are selected from the 2013 Master Sample (MS) for household-based surveys of the PSA.
II. Data Collection
The data collection was carried out from 02 May to 22 June 2022 by the 110 field teams. Each team consisted of a Team Supervisor and two to three Field Interviewers, all of whom were female. Fieldwork monitoring was an integral part of the 2022 NDHS. Regional and Team Supervisors were engaged to supervise their teams on a full-time basis. Field check tables based on data from completed questionnaires were also generated regularly by the Central Office and used to monitor progress and provide regular feedback to the field teams. GPS points were also collected during the survey. Due to the Covid-19 pandemic, guidelines were developed to mitigate potential risk of infection of field teams and survey respondents. These guidelines were followed throughout field data collection, monitoring, and supervision.
III. Methodology
The sampling scheme provides data representative of the country as a whole, for urban and rural areas separately, and for each of the country’s administrative regions. The sample selection methodology for the 2022 NDHS is based on a twostage stratified sample design using the Master Sample Frame (MSF). The MSF was constructed based on the result of the list of households from the 2010 Census of Population and Housing and updated based on the listing of households from the 2015 Census of Population. The first stage involved a systematic selection of 1,247 primary sampling units (PSUs) distributed by province or HUC. A PSU can be a barangay, a portion of a large barangay, or two or more adjacent small barangays.
In the second stage, an equal take of 22-29 sample housing units was selected from each sampled PSU using systematic random sampling. In situations where a housing unit contained one to three households, no more than three households were interviewed. In the rare situation where a housing unit contained more than three households, no more than three households were interviewed. The survey interviewers were instructed to interview only the pre-selected housing units. No replacement and no changes of the pre-selected housing units were allowed in the implementing stage in order to prevent bias.
Due to the non-proportional allocation of the sample to the different provinces/ HUCs and the possible differences in response rates, sampling weights are required for any analysis using the 2022 NDHS data to ensure the actual representative of the survey results at national level and as well as at regional level. Since the 2022 NDHS sample is a two-stage stratified cluster sample, sampling weights will be calculated based on sampling probabilities separately for each sampling stage, and for each PSU. We use the following notations:
The design weight was adjusted for household non-response and individual nonresponse to get the sampling weights for households and for women, respectively. Non-response is adjusted at the sampling stratum level. For the household sampling weight, the household design weight is multiplied by the inverse of the household response rate, by stratum. For the women’s individual sampling weight, the household sampling weight is multiplied by the inverse of the women’s individual response rate, by stratum. After adjusting for non-response, the sampling weights are normalized to get the final standard weights that appear in the data files. The normalization process is done to obtain a total number of unweighted cases equal to the total number of weighted cases at the national level, for the total number of households and women. Normalization is done by multiplying the sampling weight by the estimated sampling fraction obtained from the survey for the household weight and the individual woman’s weight. The normalized weights are relative weights which are valid for estimating means, proportions, ratios, and rates, but are not valid for estimating population totals or for pooled data.
IV. Definitions of Terms
ELIGIBLE WOMEN – All women 15-49 years old in the sample households including those visitors who stayed the night before the interview.
TOTAL FERTILITY RATES - The average number of children a woman would have by the end of her childbearing years if she bore children at the current age-specific fertility rates. Age-specific fertility rates are calculated for the 3 years before the survey, based on detailed pregnancy histories provided by women.
FERTILITY PREFERENCES - desire for another child. Women were asked whether they wanted more children and, if so, how long they would prefer to wait before the birth of the next child. Women who are sterilized are assumed not to want any more children.